
Talk:Tacrolimus
| This is the talk page for discussing improvements to the Tacrolimus article. This is not a forum for general discussion of the article's subject. |
Article policies
|
| Find medical sources: Source guidelines · PubMed · Cochrane · DOAJ · Gale · OpenMD · ScienceDirect · Springer · Trip · Wiley · TWL |
| This article is rated C-class on Wikipedia's content assessment scale. It is of interest to the following WikiProjects: | |||||||||||||||||||||
| |||||||||||||||||||||

 | Ideal sources for Wikipedia's health content are defined in the guideline Wikipedia:Identifying reliable sources (medicine) and are typically review articles. Here are links to possibly useful sources of information about Tacrolimus.
|
Clarification
[edit]Reading this I become a little confused on some items (aka I think this article could be clarified a little more than what it is at the moment). Since I'm not a medical professional (nor am I in the pharmacy profession) I'm coming to this article with just the knowledge of a 3 yr post transplant patient on this drug.
Anyway disregarding that I'll start at the introduction. I get the part where FK is introduced as both an immunosuppressent and then a topical cream but after the topical introduction "It has also been used after bone marrow transplants and for severe refractory uveitis." is somewhat thrown in there. Is the topical used after bone marrow transplants somehow, or is it used as an immunosuppressent in pill form? Same goes for the refractory uveitis. For the Contraindications and Precautions, is that for both the immunosuppressent or the topical or both? Additionally I notice it says "Black patients" (personal curiosity) under that heading, I'm curious as to why that is, it perhaps could be clarified in the article (I assume this has something to do with the topical cream and perhaps skin reactions?) Or does it even belong in there at all? I understand that a contraindication is a 'condition or factor that increases the risk involved in using a particular drug' but to include that with precautions just leaves me a bit confused, especially when seeing 'children' in there. Maybe I'm not reading that particular section right, but like I said I'm not in the medical field so..
Pretty much my last topic to hit in this section is the "Cancer risks" is this talking about the immunosuppressent or the topical or both (personally I've been warned that my skin cancer risks go up because I'm on this and a bunch of other immunosuppressents)? This doesn't really seem clear and the whole paragraph is vague at best until you get to the part about "UK dermatologists." So that's about it, I just thought I would throw that out there in case others come across this article and are as confused as I am. Although I must note that if I were to be looking for information on the medications that I take wikipedia would not be the first place I check, I just came across this article while bored and randomly typing in items to learn about. Anyway whoever clarifies this/answers these questions, thanks! --ImmortalGoddezz 23:52, 10 August 2006 (UTC)
serious drug
[edit]It would be very foolish to use this strong, possibly risky drug any more than absolutely necessary. Certainly not every day, without a damn good reason. -69.87.204.151 01:28, 3 March 2007 (UTC)
I was sad to hear about the risk a couple years ago. I used this every day for my eczema and it was the wonder drug. Doctors couldn't find anything else that worked for me. Now that I haven't used it for a couple years, I am still suffering from constant scratching from the horrible itchiness. The more I scratch the itchier it gets. Azn Clayjar 18:19, 12 April 2007 (UTC)
Antibiotic?
[edit]I think I'm going to soon edit the sentence that defines tacrolimus as a macrolide antibiotic. chemically, it is a macrolide but not an antibiotic (doesn't kill bacteria in anyway, nor is that it's aim, quite the contrary as a side effect usually).
Personal experience + Literature search
[edit]I checked out the tacrolimus page recently since I personally have pretty severe eczema and had tried Protopic soon after it was approved for clinical use. I put a test amount on the inside of my elbows and immediately felt a hot, burning sensation. This was quickly followed by an intense, unusual headache that lasted for hours. I never used the stuff again.
It was pretty disappointing, especially since the failure meant it was back to the old steroids. (Tried pimecrolimus too, and it had no effects good or bad.) Of course drug reactions depend on the individual, but I was surprised to find the industry trials had only found headaches in ~20% of patients and they wrote it off as being comparable to controls. I refuse to write the headache off as a psychological effect because I had no idea what to expect. Who'd expect to get a headache from a topical cream? Wonder why it only happens in some people? Anyway-- just did a PubMed search to back up my edits.
As I understand it the cancer risk isn't super-high, and may be specific to the species of lab animals they tested it on. Wouldn't be enough to stop me from using Protopic if it actually worked without giving me a headache. Eczema's no fun and I'd trade a few years of my life for relief.Scerevisiae 15:49, 13 June 2007 (UTC)
- Yes, I had a hot sensation too the first few times I used it, but it was nothing I couldn't handle, and I didn't get any headaches either. At that time, I really had a bad eczema but three days after using it, the condition improvided significantly, not more than a week later it was gone. I can now stretch applying the ointment to one, maybe two times in two weeks and be comfortable with my skin. I can't even remember when I applied it in once critical areas - the crooks of my arms - the last time, because they've been fine for a long time. Maybe you should give it a try for two days in spite of the side effects. Maybe they will subside. I certainly didn't have the burning sensation for a long time. --Thilo 02:45, 10 September 2007 (UTC)
- Sorry -- I know this is a page for discussing the article, not the subject -- but I've also had the burning sensation from Tacrolimus ointment: when I first used it and, bizarrely, after I've had a few sips of beer, but only if it's real ale! All I can think is that I'm having some kind of allergic reaction to the beer and that reaction is being modified by the Tacrolimus. Sam Dutton (talk) 22:17, 28 February 2008 (UTC)
- Alcohol sensitivity is listed as one of the clinically significant side-effects. Also experienced headache and burning, similar to the feeling after too much sun. — Preceding unsigned comment added by 66.57.73.215 (talk) 20:47, 1 January 2014 (UTC)
Trying to add reference
[edit]Sorry to ask, but I'm terrible at adding references. Mine in particular is for tactrolimuses use in treating ulcerative colitis. If anyone would be so kind as to add this link as a reference to this use it would be greatly appreciated:
http://www.springerlink.com/content/g2kjwecu3dthb3l2/
I have some other sources for its use against UC if this one is not sufficient enough.
DO NOT USE PROTOPIC FOR ECZEMA!!
[edit]DO NOT USE PROTOPIC!! I AM SERIOUS!! http://www.washingtonpost.com/ac2/wp-dyn/A17568-2005Feb11?language=printer
instead, use vanos for strong eczema, cloderm for medium, and atopiclair (non-steroidal) for mild eczema. i have eczema too. also, use herb medicene if you want to cure it "safely." XU-engineer 13:40, 11 August 2007 (UTC)
- That article talks largely about children and excessive use of the drug. The kid mentioned hat the ointment applied over the whole skin area of his body (!!). I only need very small amounts in select parts of my body to stay exczema-free so I think the cancer risk is not too high. Your suggestion on the other hand shines in another light if you consider that Vanos and Cloderm actually are steroids and if you read this: http://www.medscape.com/viewarticle/527690
- Due to a lack of long-term safety data and the potential for suppression of the hypothalamic-pituitary-adrenal axis, treatment should be limited to 2 consecutive weeks at a maximum dose of 60 g per week. Therapy should be discontinued when control of the skin condition has been achieved. A patient's diagnosis may require reassessment if the condition does not improve after 2 weeks
- With me, Protopic works as well as steroids but without the skin thinning and other side effects that these steroids have. At the moment, I am willing to live with the risk of applying Protopic, as it really does help me at least. --Thilo 02:56, 10 September 2007 (UTC)
- Tacrolimus is not intended for prolonged use on large areas of the body. Every time I have been prescribed Tacrolimus, I was given specific instructions, where, when and how to apply it, to minimise such risks. If those people had listened to their doctor's advice, I'm sure the cases wouldn't have occurred. 87.102.78.143 (talk) 23:46, 2 September 2010 (UTC)
Discovered in 1984 and 1987?
[edit]From the first paragraph: "It is a 23-membered macrolide lactone discovered in 1984". From the second paragraph: "Tacrolimus was discovered in 1987 by a Japanese team". Neither of these assertions are sourced. (I have undergone two liver transplants, and tacrolimus/Prograf is my primary immunosuppressant.) Emptyshell 04:52, 3 October 2007 (UTC)
- From the "answering my own question" department: 1984 is the correct date, according http://www.prograf.com/HCP/Prograf_History.htm. Emptyshell 04:55, 3 October 2007 (UTC)
Severe atopic dermatitis
[edit]I, for one (in the UK), don't have 'severe atopic dermatitis', but I'm being treated with Tacrolimus.
Maybe the first paragraph should be changed to 'moderate to severe atopic dermatitis'?
Sam Dutton (talk) 22:21, 28 February 2008 (UTC)
IUPAC Name and structure
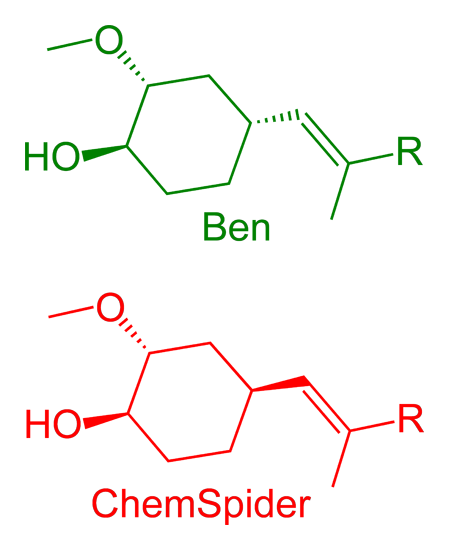
[edit]I believe the structure has the wrong stereochemistry and this is the correct structure
http://www.chemspider.com/Chemical-Structure.4976056.html
The name is: (3S,4R,5S,8R,9E,12S,14S,15R,16S,18R,19R,26aS)-5,19-dihydroxy-3-{(1E)-1-[(1S,3R,4R)-4-hydroxy-3-methoxycyclohexyl]prop-1-en-2-yl}-14,16-dimethoxy-4,10,12,18-tetramethyl-8-(prop-2-en-1-yl)-5,6,8,11,12,13,14,15,16,17,18,19,24,25,26,26a-hexadecahydro-3H-15,19-epoxypyrido[2,1-c][1,4]oxazacyclotricosine-1,7,20,21(4H,23H)-tetrone --ChemSpiderMan (talk) 00:41, 30 May 2008 (UTC)
- I looked at both images, but they're oriented differently. Which aspects of the stereochemistry of the current image are wrong?
- Thanks for finding this error.
- Ben..please contact me offline at infoATchemspiderDOTcom with your email address and I will send you the molfile in an attractive format for uploading.--ChemSpiderMan (talk) 23:59, 30 May 2008 (UTC)
3D or 2D molfile? I've got the 3D structure from the x-ray study - will this be the same?
Have emailed you.
Cheers
Ben (talk) 00:04, 31 May 2008 (UTC)
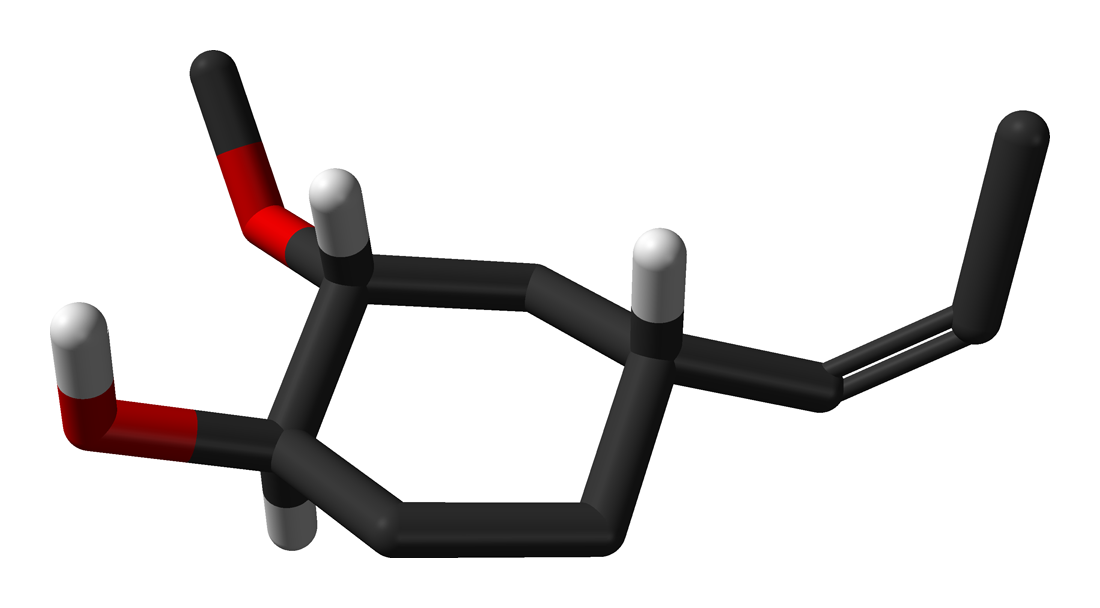
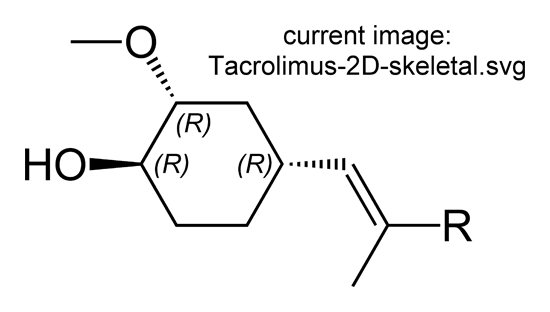
- I put the systematic name you provided above into ChemDraw and compared it with the structure in my Image:Tacrolimus-2D-skeletal.png. They differ in the stereochemistry at one particular carbon. I've made a comparison here. I believe my structure is correct (and therefore the name given above is wrong), based on the x-ray crystal structure of tacrolimus complexed to a protein in PDB file 1bkf - compare the skeletal structures of the disputed fragment with the 3D structure of the fragment from 1bkf.
{kind=link}
{kind=link}
{kind=link}
- I may, however, have made a mistake in interpreting the information here, so it'd be great if several people could check.
- Cheers again
- Ben, take a look at the image shown on [this DailyMed page http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=2958]. Let me know what you think--ChemSpiderMan (talk) 06:06, 31 May 2008 (UTC)
- I've found the same structure but from a more reliable source: Acta Cryst. (1995). D51, 522-528.
- Both of these structures are have the same stereochemistry same as my image at the fragment in question, i.e. the R group and the MeO group are both pointing in the same direction, while the OH group is pointing in the opposite direction.
- Looking at the ChemSpider structure again, now that we've identified the part we think if different, the Chemspider structure is also correct - and identical. It's just the name given above.
- How did you come to the conclusion that the image in this article was wrong? Was it due to the name? If so, there might not be a mistake after all.
- I think I caused confusion with my initial comment. The name I posted above was for the structure in WIkipedia already. The CORRECT name I believe is:
(1R,9S,12S,13R,14S,17R,18E,21S,23S,24R,25S,27R)-1,14-dihydroxy-12-{(1E)-1-[(1R,3R,4R)-4-hydroxy-3-methoxycyclohexyl]prop-1-en-2-yl}-23,25-dimethoxy-13,19,21,27-tetramethyl-17-(prop-2-en-1-yl)-11,28-dioxa-4-azatricyclo[22.3.1.0~4,9~]octacos-18-ene-2,3,10,16-tetrone In terms of how I concluded the article was wrong it was not using the name. It was by careful visual inspection of every structure as part of the curation process. See here: http://www.chemconnector.com/chemunicating/dedicating-christmas-time-to-the-cause-of-curating-wikipedia.html I AGREE with this observation: the R group and the MeO group should both be pointing in the same direction, while the OH group is pointing in the opposite direction. —Preceding unsigned comment added by ChemSpiderMan (talk • contribs) 15:49, 31 May 2008 (UTC)
- See also this.
{kind=link}
- So does that mean there's no problem with the current image?
- Cheers
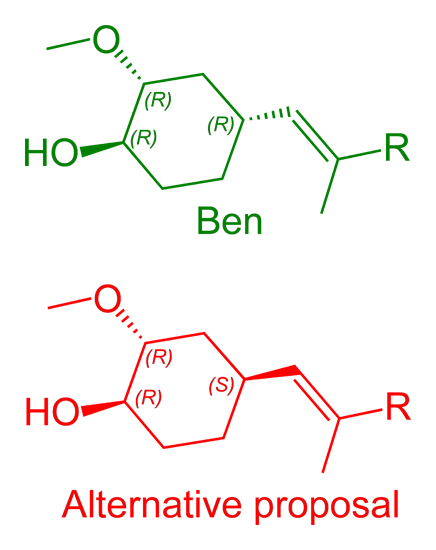
- Sorry...I am recovering from surgery yesterday and not clear minded right now. My comment should have been "the R group and the OH group should both be pointing in the same direction, while the OMe group is pointing in the opposite direction." According to my view this would give R,R,R. The present way on the image gives R,R,S.--ChemSpiderMan (talk) 03:37, 1 June 2008 (UTC)
Sorry to hear about your surgery, best wishes for a speedy recovery.
I still believe the current image has the correct (R),(R),(R) stereochemistry: see this image annotated with stereo, stereo calculated automatically in ChemDraw. However, the current image would better if the hashed bonds were wedged, to show their directionality, in line with the 2006 IUPAC guidelines, and as I did when I made the 2D original.
{kind=link}
The crystal structure shows that the R and the OH are not pointing in the same direction
Ben (talk) 13:54, 1 June 2008 (UTC)
- I'll send you a couple of structures via email to take a look at and comment on. You may be right and it might be an issue of the wedge direction since wedges can kill stereo detail.--ChemSpiderMan (talk) 01:16, 2 June 2008 (UTC)
Patent expiry dates - generics ?
[edit]tacrolimus : US patent 5,260,301 expired in Feb 28, 2011 - Not sure what it actually covers though. Rod57 (talk) 22:49, 1 March 2011 (UTC)
Also USP 5,385,907 expires Jan 31, 2012 . - Rod57 (talk) 03:18, 8 February 2012 (UTC)
- USP 8,551,522 and USP 6,440,458 both expire March 2019.
- Article mentions "alternative brands" are these generics ? or what are the prospects of generic tacrolimus ? - Rod57 (talk) 13:45, 26 March 2019 (UTC)
Who makes it
[edit]I am currently taking Tacrolimus for liver transplant; I am in rejection and terminal; I am looking for the pharmaceutical company who makes this drug as I can no longer afford the co-pay for procuring this drug, can you help? — Preceding unsigned comment added by 69.242.224.125 (talk) 16:27, 12 August 2013 (UTC)
Heart transplant patient: Switching from cyclosporin (after using 18 years) to Tacrolimus or to some other?
[edit]Wiki says now: "It has similar immunosuppressive properties to cyclosporin, but is much more potent. Immunosuppression with tacrolimus was associated with a significantly lower rate of acute rejection compared with ciclosporin-based immunosuppression (30.7% vs 46.4%) in one study. Clinical outcome is better with tacrolimus than with ciclosporin during the first year of liver transplantation. LONG-term outcome has not been improved to the same extent". QUESTIONS:
- What if a person who has had heart transplant for 18 years and has used Cyclosporin for 18 years switches to Tacrolimus?
Is the outcome better then?
- A long time patient may need to switch because Cyslosporin damages kidneys.
Is Tacrolimus safer for kidneys?
ee1518 (talk) 16:52, 4 July 2015 (UTC)
FK
[edit]What is the FK protein naming scheme? If you Google "FK505", "FK504", etc they exist, but what does "FK" stand for? 92.184.117.163 (talk) 14:33, 18 December 2022 (UTC)
FK506 as alternative name
[edit]In my view, the name FK506 should be included in the lead (not solely in the infobox), because it is NOT an obsolete or former name. For example, it is used as the primary name in this 2023 paper. Robert.Allen (talk) 19:44, 21 January 2023 (UTC)
- User:Whywhenwhohow: WP:PHARMOS is a guideline, not a rule, and in this particular case should not apply. Adding the name FK506 does not clutter the lead. Moreover, FK506 is no longer just a "development name", since it is still frequently used in the research literature as the primary name of the compound and is also part of the name for FK506 binding proteins. For examples, see [1], [2], [3], [4], [5], [6], [7]. It is easy to find many more examples in the recent literature where FK506 is used and tacrolimus is not. --Robert.Allen (talk) 22:43, 21 January 2023 (UTC)